Jessica Pin is a US advocate with the goal of comprehensive and equitable coverage of the clitoral anatomy in Obstetrics & Gynaecology (OB/GYN) textbooks. She’s regularly interviewed by the media on this topic and her study was published in the Aesthetic Surgery Journal. Our editor, Ginger Gorman, had a long conversation with Jessica about her goals, thoughts, experience and activism in this area.
Tell us the personal back story. Who are you? How did you become an activist concerned with equitable coverage of the clitoral anatomy? And what do you mean by “equitable”?
When I was 17, I stumbled upon false, stigmatizing information about labia minora published by doctors online while trying to learn what a clitoris was. I had never been taught about the vulva, clitoris, or labia minora in sex ed. After seeing labiaplasty advertisements and spurious claims that protruding labia minora are considered “unfeminine and embarrassing” and are caused by sexual activity, masturbation, male hormones, and aging, I felt ashamed that my labia minora stuck out. Because I also read that labiaplasty involved no risks to sexual function, I had surgery within days of turning 18.
A renowned OB/GYN surgeon, who has held multiple leadership positions and been given the highest awards by his peers, was recommended to my plastic surgeon father by the head of the OB/GYN department. He completely amputated my labia minora and severed the dorsal nerves in my clitoris in a clitoral hood reduction done without my consent, robbing me of clitoral sensation permanently. I say “permanently,” but they probably could have been repaired if the injury had been acknowledged early enough. Instead, I was told my loss of sensation was not possible and that I just needed to relax and/or fall in love.
I knew I was not crazy, so I taught myself the anatomy. I was studying pre-med biomedical engineering with a bioelectric focus, so I accidentally minored in electrical engineering as well. Nerves are a lot like wires. One class I took was focused entirely on nerves. I could say this all made me equipped to notice the gap in anatomy education. But the truth is it didn’t. What made me notice was simply curiosity, a willingness to question authority, and a determination to prove what happened to me was not all in my head.
Anyone can teach themselves what a nerve is. Anyone can look up studies of nerves in the clitoris. Anyone can see the nerves in the clitoris were missing from OB/GYN textbooks prior to 2019 and that they were missing from most anatomy textbooks as well. We focus so much on credentials, and people think if you don’t have the right credentials, you have no right to an opinion. But with enough intelligence and drive, anyone can teach themselves anything. When it comes to what is true or false, a commitment to providing evidence rather than asserting authority should be the basis for credibility.
By “equitable,” I mean that my goal is to get the anatomy of the clitoris covered in the same depth as that for other organs. For example, the nerves in the penis are always included in anatomy resources. The nerves in the clitoris are just as large. They are just as important. They should be included as well. That they aren’t is fundamentally a matter of censorship caused by taboo, as well as a denial of the importance of female sexual response to overall health and to relationships.
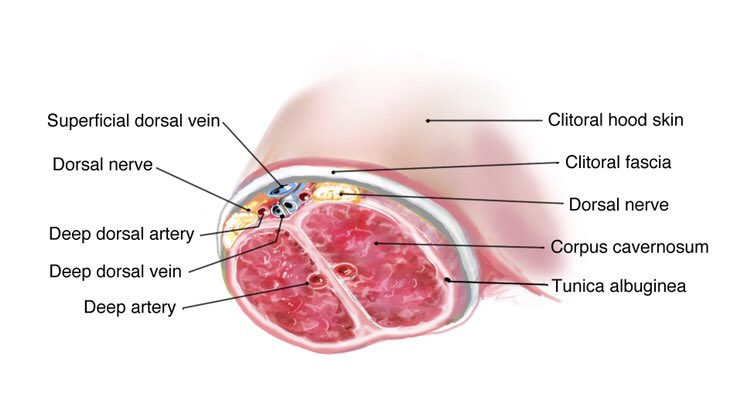
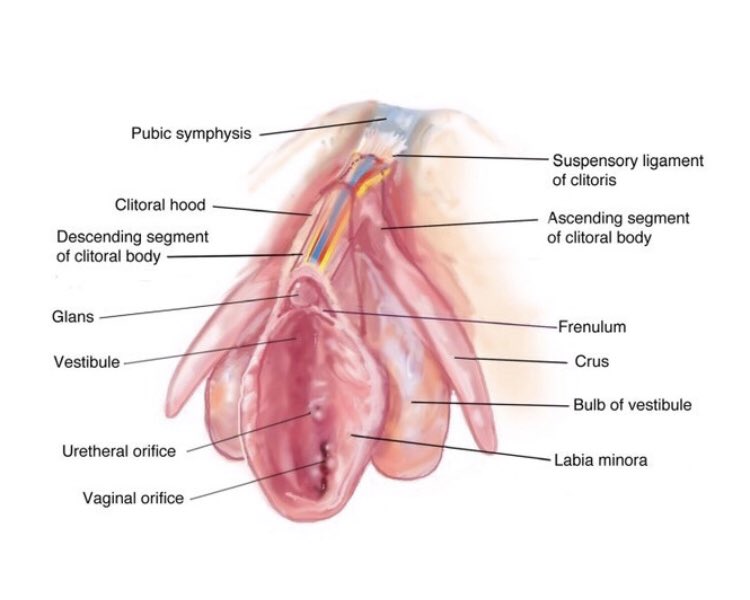
Jessica wants correct clitoral anatomy, including nerves, to appear in all medical textbooks. Pictures: Supplied.
I note you’ve previously said that in an ideal world cosmetic labiaplasty or any form of female cosmetic genital surgeries should not be done. Why have you come to this view? What’s your concern with sexual sensation and labiaplasty?
Cosmetic surgery is ethical if and only if there is informed and autonomous consent, a reasonable standard of care, and a reasonably low rate of functional complications. Maybe in an ideal world where these conditions are met, female genital cosmetic surgery would be ethical. However, in our actual world, these conditions are nowhere near met.
Labiaplasty surgeons call protruding labia minora “hypertophy.” This means “excessive growth” and implies pathology. By calling all protruding labia minora “hypertrophic” they use their medical authority to stigmatize and pathologize half the female population. This is misleading and thus coercive.
Additionally, labiaplasty surgeons set standards for what is considered “ideal” without any possible pushback from society at large due to modesty standards in everyday life. We don’t walk around with our vulvas visible. Vulvar aesthetics are not a common topic that comes up.
There’s very limited ability to push back on standards surgeons set. In my opinion, this beauty standard isn’t even real. The labia minora develop during puberty and atrophy with menopause. They also engorge with arousal. From an evolutionary standpoint, it makes no sense for an aesthetic that signals fertility and arousal to be considered unattractive.
Labiaplasty surgeons also publish blatant medical misinformation about labia minora. They publish, online and in peer reviewed medical journals and textbooks, that labial hypertrophy is caused by excess androgens, sexual activity, masturbation, and aging. They also associate labial hypertrophy with urinary incontinence and infections. None of these claims, which serve to stigmatize large labia minora, are backed by any evidence.
Labiaplasty surgeons also advertise labiaplasty and clitoral hood reductions with fraud. They claim labiaplasty is “rejuvenation” – that it will restore a youthful appearance. But smaller labia minora are not more youthful unless we are talking about actual children. 10 normative studies have shown no positive correlation between age and labia minora size. Surgeons similarly advertise that clitoral hood reduction can improve function, but there is no evidence, and the reality is it can result in loss of clitoral sensation.
Risks additionally are severely minimized and sexual function is not reasonably considered in literature on female genital cosmetic surgery. The top labiaplasty surgeon in the US, Dr. Gary Alter, has published in the Aesthetic Surgery Journal, the top journal in the world, that there is “no evidence” the labia minora are involved in sexual response. This is absolutely false.
The dorsal nerves of the clitoris were not mentioned anywhere in female genital cosmetic surgery literature until 2015, over a decade after mine were severed. Surgeons had simply not considered them. To this day, expert female genital cosmetic surgeons describe their course incorrectly on RealSelf (a UD website where you can search for a doctor for elective cosmetic treatment) in the context of misinforming patients about risks and gaslighting patients who have lost sensation.
Finally, unlike the case with other cosmetic surgeries like breast reduction and rhinoplasty, there are no training standards for female genital cosmetic surgery.
Female genital cosmetic surgery is not covered, according to any standard set by governing bodies, in residency for either OB/GYNs and plastic surgeons. Realistically most surgeons performing these procedures are doing surgeries they were never trained to do on anatomy they were never taught.
Even if labiaplasty is performed as safely as possible, there will always be a removal of sexually sensitive tissue. The labia minora have the same types of nerve endings as the clitoris, engorge with arousal, and are actively involved in sexual response. Another thing few people talk about is how the labia minora mechanically facilitate stimulation of the clitoris. Back in 2007, one of the first things I searched for was “vulvar biomechanics.” There was nothing. There is still nothing. Why are surgeons operating on anatomy whose function medicine hasn’t bothered to understand?
Also, clitoral hood reduction is fundamentally clitoral surgery. Most of the clitoral hood is actually just the skin of the clitoris itself. The dorsal nerves of the clitoris are just beneath. But how many women would consent to clitoral hood reduction if they understood it to be a surgery on the clitoris?
Finally, given that female genital cosmetic surgery necessarily involves functional tissue, removing it for aesthetic purposes is ethically contentious even under the best conditions. What does it mean when women are asked to choose between prioritizing function and prioritizing aesthetic with anatomy as intimate and as critically important to our quality of life as our vulvas?
I have seen teenagers comment that they would rather lose clitoral sensation that have an ugly vulva. And this raises concerns. Most people would not, for example, agree to letting patients consent to remove or even partly remove healthy limbs if they so choose. At the very least, I can imagine the public objecting to limb amputation advertisements.
Why do you focus on changing textbooks, rather than changing medical organisations? (Please also explain why you think medical orgs are resistant to change?
I targeted professional medical organizations first and I couldn’t get them to acknowledge any problem with education or training. Leadership at the American Board of OB/GYN assured me there was no problem. They insisted I was mistaken about anatomy being missing. The American Council on Graduate Medical Education similarly assured me they looked into it and I was mistaken. They assured me OB/GYNs were in fact being taught anatomy that was nowhere to be found in their textbooks or journals. No one at the American College of OB/GYNs would even respond to me.
I now regret not also contacting leadership at the American Society of Plastic Surgeons and the American Board of Plastic Surgeons at that time, and I presently have been asked to not discuss them. But my memory is the anger and frustration I felt trying to solve the problem of getting OB/GYNs educated was exhausting enough as is. So I focused on OB/GYN first to keep things manageable for myself, as I personally was harmed by an OB/GYN.
I also tried meeting with the Chief Medical Officer and the Head of Patient Safety at a local hospital. The Chief Medical Officer ironically suggested I start a #metoo movement for women harmed by female genital cosmetic surgery. I told him that would never work. Back then, even I never thought I would share my story. I still haven’t gotten anyone else to do it. It is an especially intimate matter. The combination of bodily violation, permanent disability, sexual nature, and vulnerability to victim-blame makes this exceedingly difficult. However, that did influence my later decision to take my advocacy to social media.
I also contacted the Association of American Medical Colleges. I got nowhere with them. I contacted anatomy professors, residency program directors, and department heads. I contacted doctors who had shown some interest in the clitoris and female genital cosmetic surgeons who seemed more ethical than most. They were either cynical or uninterested. Those who agreed anatomy education needed to be improved didn’t know how to make it happen. I also crashed the Annual Meeting for the American College of OB/GYNs and passed out flyers, looking for OB/GYNs interested in getting clitoral anatomy disseminated. Discouragingly, that did not work at all.
I honestly had no idea what I was doing. It’s just that for 7 years, I’d needed to do something, and for the longest time, I put it off because I didn’t know how, and I was afraid of what would happen. I was afraid I would fail. And I was afraid if I did fail, that would mean the world thought my trauma wasn’t worth preventing. In retrospect, I was taking things too personally, as if my dignity as a human being were on the line, but that’s why I was so afraid. And that’s why once, I started, that meant doing anything and everything I could figure out to do. I made a lot of mistakes, and I would do things differently if I could start over now, but there is a lot to be said for just getting started, even if that means misstepping.
So contacting textbook authors was one strategy I tried that has worked well. At first, it didn’t seem like anyone listened to me. But I got better at writing emails requesting updates, and once updates came out, I could use the new updates to persuade other textbook editors to update as well. This was an indirect way to influence OB/GYN education. I also contacted OB/GYNs to see if anyone would be interested in publishing a study to get the anatomy into a major OB/GYN journal where OB/GYNs would read it. I published my study in a plastic surgery journal with my plastic surgeon father for this purpose as well.
While the most efficient way to get training and education standards changed is through professional medical organizations, their cooperation has been limited. The American Board of OB/GYN did finally add detailed clitoral anatomy to their maintenance of certification program last year. But it is only optional learning that counts towards maintaining board certification in OB/GYN. It is not required.

Although Jessica has made significant change when it comes to correct representation of clitoral anatomy, not everyone is pleased about her activism. Picture: Supplied
What responsibility to doctors have in all this?
Despite the American Medical Association’s Code of Ethics stipulating that doctors report irresponsible or harmful practice by colleagues, most doctors only feel responsible for how they treat their own patients. This is a problem because it makes it very difficult to get harmful standards of care changed.
Doctors practicing in negligent ways won’t want to recognize any error or fault. And doctors who see them practicing in negligent ways won’t want to speak up. Not speaking up when patients are harmed or when preventable risk factors are very obvious is very much a part of medical culture. At least here in the US, medicine is self governing and self policing. But there is a great deal of bias and willful blindness that makes this inviable.
If we look back in history, why is our societal interest in – and knowledge of – female anatomy so poor?
Widespread ignorance about vulvar anatomy stems from cultural suppression of female sexuality.
There is a belief that the vulva is not reproductive. Yet we know that the vulva, including the clitoris, is responsible for most female sexual pleasure. And we know that sexual pleasure is the number one reason human females have sex. Certainly not many human females would choose to reproduce outside of cultural systems of coercion if they did not experience pleasure. As such, organs responsible for our pleasure are fundamentally responsible for motivations to engage in reproductive behavior.
But there is this separation of female sexual pleasure from reproduction that is fundamentally a denial of female sexual agency.
Watching your social media, I see you are often having small and big wins, and gradually changing things (Congratulations!). How would you encapsulate the changes you’ve made? How far have we got to go?
Honestly, my goal is to just get the ball rolling enough that it will keep rolling without me pushing it. Depending on whether professional medical organizations in plastic surgery and OB/GYN will take action, it could be years before surgeons considered qualified to operate on vulvas can be trusted to know the surgical anatomy. It could be decades.
The reason I am so cynical is because, while getting textbooks updated will change education for the next generation of surgeons, it does nothing for the surgeons who are currently in practice and operating on vulvas. Unless professional medical organizations take action, currently practicing doctors will need to retire before we can count on a reasonable standard of care.
Recently I have been more focused on the preponderance of misinformation about vulvas and how this precludes informed consent. I have made very little progress with this. I have gotten the ASPS to stop calling labiaplasty “rejuvenation.” And I got the Aesthetic Surgery Journal to retitle their section on genital cosmetic surgery so they are no longer calling it “Genital Rejuvenation.” Like I said, this is fraud, and it is fraud that many major medical institutions, including Stanford Medical School, are engaging in.
What would complete success look like to you? How would this change medicine and women’s experience of it?
Complete success will be achieved when vulvas are treated like other parts of the body; when surgeons operating on vulvas know the anatomy involved, when there are training standards for vulvar surgeries; when anatomy of the clitoris is complete and correct in all anatomy textbooks, OB/GYN textbooks, urology textbooks, and female genital cosmetic surgery textbooks; when clitoral anatomy is considered general anatomy and taught to all medical students; when anatomy and physiology involved in female sexual response is as well studied as anatomy and physiology involved in male sexual response; when female sexual medicine has as much anatomic and scientific basis as male sexual medicine does; when stigmatizing misinformation about vulvas is no longer rampant; when surgeons are no longer advertising female genital cosmetic surgeries with fraud; where female sexual function is taken seriously and considered medically important.
My hope is that once these goals are reached, women will not lose sexual function due to the ignorance and incompetence of medical providers. I hope also that women who do suffer any loss of sexual function from any injury will be taken much more seriously than I was. The function of the vulva, including the clitoris, should be properly evaluated before doctors conclude sexual dysfunction has some psychological cause. This simply isn’t happening now. And it is gaslighting.
Someday, female sexual health, which includes that anatomic and physiological capacity for pleasure, will hopefully be considered a human right. Women will be as entitled, as patients, to seek help with sexual function as men are today. And sexual and reproductive functions will be considered overlapping for women as much as they are for men.
Your focus seems mainly on the US. Has your work impacted other countries too?
Ann Augur, who lives in Canada, is one of the top anatomists in the world. She edits three major anatomy textbooks, all of which will contain in-depth anatomy for the clitoris in upcoming editions. She is also behind the 4 new illustrations of clitoral anatomy that have been added to the Wolters Kluwer Female Reproductive System Posters.
Though I have not had luck with Gray’s Anatomy, published in the UK, my hope is that I’ve engaged enough with the chief editors of Gray’s Surgical Anatomy and Gray’s Anatomy: Anatomical Basis for this to have some impact on next edition.
Rohen’s Photographic Atlas of Anatomy is published in Germany. Because I have not been able to connect with them directly, I had an editor at Wolters Kluwer reach out. Originally, she seemed certain changes would be made. Now she just says they are being “considered.” It is a book of dissection photos, so cross your fingers that they will show dissections of the clitoris that are as complete as those for the penis in the next edition.
Many popular textbooks are used internationally and translated into other languages. For example, I changed Te Linde’s Operative Gynecology. I’ve noticed there is also a South Asian edition, but it has not been updated yet. The editors of Netter Atlas of Human Anatomy have also let me know they have updated several illustrations for their upcoming edition. And Netter is published in 16 languages and used all around the world.
Is there anything else you’d like to say?
Please share any illustrations of clitoral anatomy to help spread awareness and knowledge. What is shown and normalized cannot be considered so taboo it is censored from anatomy education. Also, please let women with labia minora that stick out that they are beautiful too. And please discourage supporting a field of surgery that has not bothered to take reasonable precautions to avoid genital mutilation.
Ginger Gorman is a fearless and multi award-winning social justice journalist and feminist. Ginger’s bestselling book, Troll Hunting,came out in 2019. Since then, she’s been in demand both nationally and globally as an expert on cyberhate and the real-life harm predator trolling can do. She's also the editor of BroadAgenda and gender editor at HerCanberra. Ginger hosts the popular "Seriously Social" podcast for the Academy of the Social Sciences in Australia. Follow her on Twitter.





